By R. Bot, A. Tirla and Simona Cavalu
Background and Clinical Significance: Vascular complications occurring in the context of trans-trochanteric fractures are rare (mean incidence 0.2–0.5%) but can be fatal if not recognized and treated promptly. Most of the previously reported vascular injuries are iatrogenic, and various mechanisms of injury and producing agents have been reported. Case Presentation: We present a rare but severe vascular complication following proximal femur fracture fixation in the case of a 77-year-old patient, specifically, a deep femoral artery injury after DHS osteosynthesis. CT angiography identified the lesion in the territory of the profunda femoris artery, precisely at the level of the most distal screw, suggesting over-drilling as the underlying cause. The case is presented in the context of a literature review, updating the most important features of the vascular complications, incidence, diagnosis and treatment. Conclusions: This case highlights the critical role of early diagnosis and prompt interdisciplinary collaboration between orthopedic and vascular surgeons in managing iatrogenic vascular complications, achieving a favorable outcome. Copyright Simona Cavalu et al.
lateral view. Copyright Simona Cavalu et al.
The radiological examination reveals a per-trochanteric comminuted fracture with medial displacement of the lesser trochanter and atherosclerosis of the deep femoral artery.
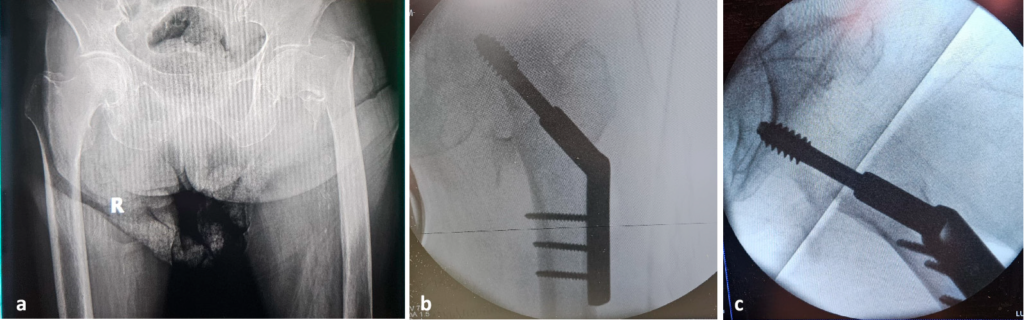
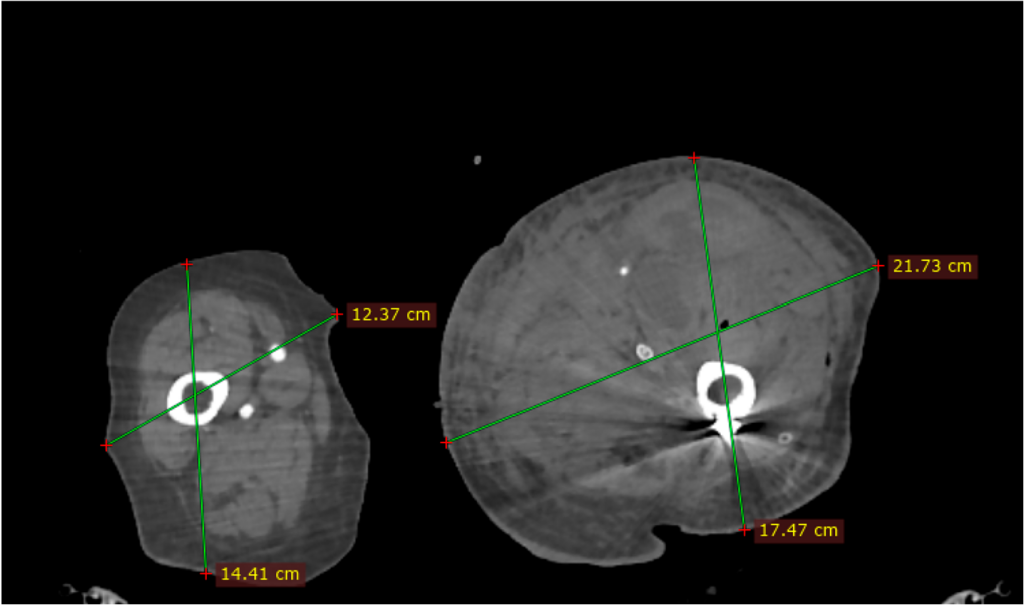
Angio-CT investigation was performed, identifying a lesion in the deep femoral artery, within the area of the most distal screw.
Simona Cavalu et al.
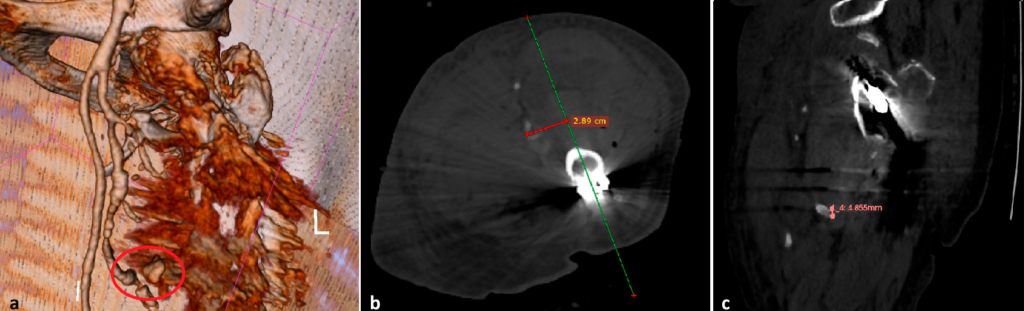
extravasation (red circle); (b) the distance between the screw trajectory (green line) and the profunda femoris artery lesion, axial view (red line); (c) the distance between the vascular lesion and screw direction, sagittal view. Copyright Simona Cavalu et al.
Most vascular injuries associated with proximal femur fracture fixation were reported in intertrochanteric fractures treated with either dynamic hip screws or intramedullary nails. The deep femoral artery was by far the most frequently affected vessel, accounting for more than half of all lesions, followed by the superficial and common femoral arteries. Intrapelvic injuries were uncommon (<10%). The majority of cases were iatrogenic, mainly related to over-drilling or excessively long screws, while displaced lesser trochanter fragments were also an important cause. Pseudoaneurysms represented the predominant type of vascular lesion,
whereas arteriovenous fistulas were rare but well-documented, usually between the deep femoral artery and vein. The International Surgery Journal (2023) also reported a profunda femoris artery pseudoaneurysm following dynamic hip screw fixation for an intertrochanteric fracture. Additional recent case reports also confirm pseudoaneurysms as the most frequent vascular lesion after hip fracture fixation. Overall, almost all patients required surgical or endovascular repair, with conservative management being exceptional. Copyright Simona Cavalu et al.
Preventive Considerations
- Preoperative vascular assessment—Patients with visible arterial calcifications on radiographs or known vascular comorbidities may benefit from preoperative vascular imaging, such as Doppler ultrasound or CT angiography, to evaluate arterial proximity and fragility.
- Management of the lesser trochanter fragment—In cases with significant medial displacement, surgical reduction or excision of the lesser trochanter can reduce the risk of delayed arterial erosion, particularly of the deep femoral artery.
- Instrumentation control—The use of drill stops, proper intraoperative measurement of screw length, and multiplanar fluoroscopic verification during implant placement are essential to prevent arterial penetration.
- Postoperative surveillance—A sudden drop in hemoglobin levels, expanding hematoma, or persistent thigh pain should prompt immediate imaging evaluation (Doppler ultrasound or CT angiography). Clinicians should also be aware that beta-blocker therapy may mask tachycardia, potentially delaying recognition of internal bleeding.
- Interdisciplinary collaboration—Early involvement of vascular surgeons and imaging specialists is strongly recommended in suspected or confirmed cases to ensure timely diagnosis and appropriate management. Copyright Simona Cavalu et al
Full text at https://doi.org/10.3390/reports8040191